In the last five years we’ve seen a major increase, not only in immunotherapy trials in oncology, but also in immunotherapy approvals. It’s an exciting time to be working with the immune system!
Medelis has been managing immunotherapy studies in oncology since 2008. We work directly with sponsors on the development of clinical strategy (protocol, endpoints, regulatory) and with study execution in this growing field.
This article is written for Chief Medical Officers, researchers and all of those focusing on continuing development in this field. It is based on Dr. John Grous’ presentation from our webinar: How Immune-Related Response Criteria Is Changing Immunotherapy Treatments.
To start, let’s do a quick review of the current research regarding neoplastic diseases.
Hanahan and Weinberg in 2000 proposed that six hallmarks of cancer together constitute an organizing principle that provides a logical framework for understanding the remarkable diversity of neoplastic diseases:
It seems every year these hallmarks increase, and in 2011 they updated their paper to identify four additional hallmarks:
For an anticancer immune response to lead to the effective killing of cancer cells, a series of steps must be initiated and allowed to proceed and expand. These steps are referred as the Cancer-Immunity Cycle.
Here is a diagram of the process:
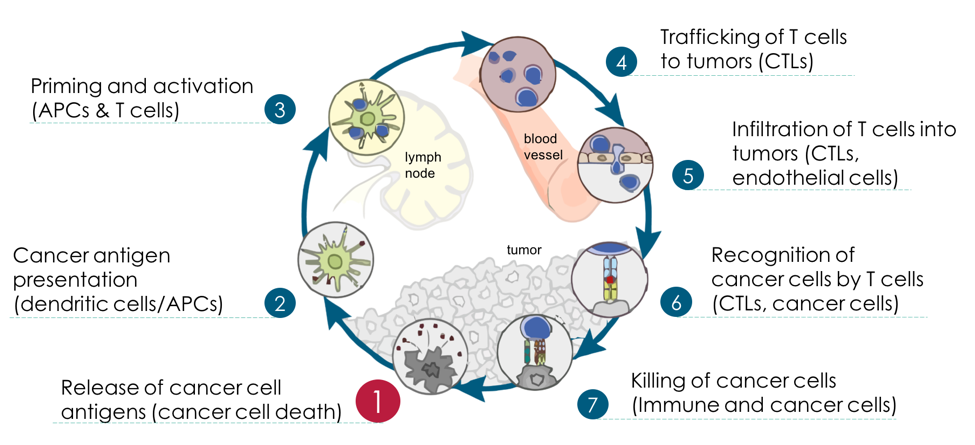
As you know, there is an innate immune system based on pattern recognition, receptors and toll-like receptors, and also immunity that involves the generation of antibodies through B-cell responses.
Essentially the generation of CTLs (Cytotoxic Lymphocytes) involves a recognition of either tumor-associating antigen or foreign antigen that’s recognized by dendritic cells. There is processing that occurs within the cell so that, over time, the dendritic cell or antigen-presenting cell will modify your antigen through the MHC complex and present the antigen to the T cell receptors. Besides the T cell priming, in addition to the presentation of the antigen, you need co-stimulatory molecules and the right cytokines environment.
For the adaptive immune system to function properly, T cells require three signals to be fully functional killers:
Below is a description showing the process starting from signal 1, where it is recognized by tumor cells, through the process of dendritic cell processing and T cell presentation through generation of CTLs that invade the tumor.
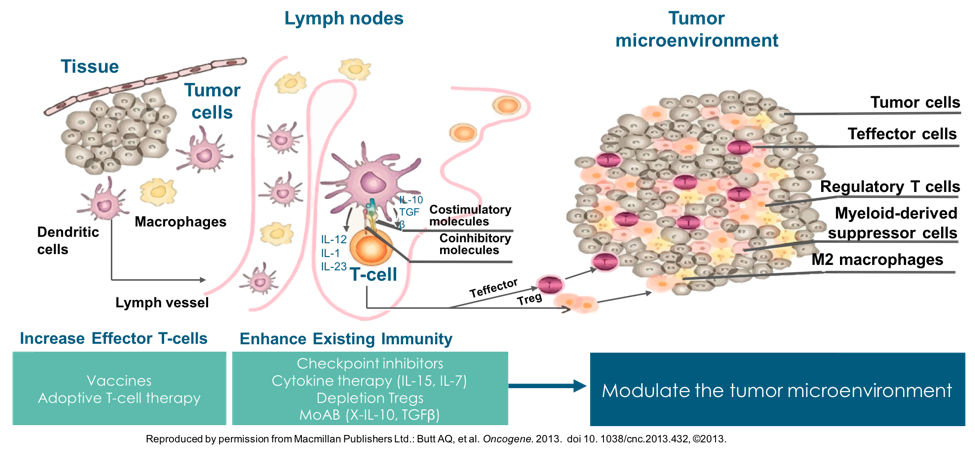
The process can be enhanced by checkpoint inhibitors — cytokine therapy (IL-15, IL-7) — and the lack of inhibitory cytokines, like IL-10 AND TGFβ that are mainly secreted by Tregs that inactivate the CDB CTL.
Regarding Tregs, it’s important to note that all Tregs are not the same. There is a subset of Tregs that have tumor-suppressor properties. The main phenotype for Treg is CD4, CD25 and Fox P3. Out of that phenotype, a third are tumor-suppressors and the rest are either involved in inflammation or are not even inducible.
It’s interesting to note that there is a chemokine receptor on the suppressor Tregs, called CCR4 (Chemokine Receptor 4), which is involved in trafficking these Tregs from lymph nodes to tumor environments. CCL22 and CCL17 induce this trafficking. There’s an antibody to this that’s actually approved in Japan, and it seems like CCR4 is also expressed on T cell lymphomas and T cell leukemia. The antibody is approved as a single agent for these leukemia and has an activity of 20-25%. It’s currently in phase III trials for cutaneous T cells lymphoma. The other action it has (in preclinical models) is that it can actually deplete Tregs.
Along this pathway are numerous stimulatory and inhibitory factors in the Cancer-Immunity Cycle. I won’t address them all here, but it’s worth noting the CTL4 immune checkpoint in Step 3 and also the anti-PD-L1 checkpoint in Step 7 at the tumor environment.
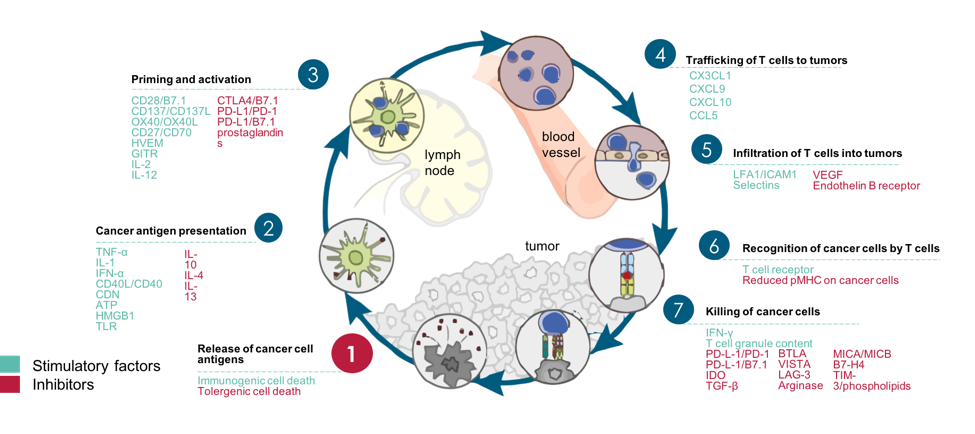
The T cell has various inhibitory receptors and stimulatory receptors. In fact, some receptors share the same ligands, e.g., CTL4 with B7 and CD28 with B7. (We’ll address these in greater detail in a future article.)
The numerous factors that come into play in the Cancer-Immunity Cycle provide a wide range of potential therapeutic targets. Here are examples of some of the therapies currently under preclinical or clinical evaluation.
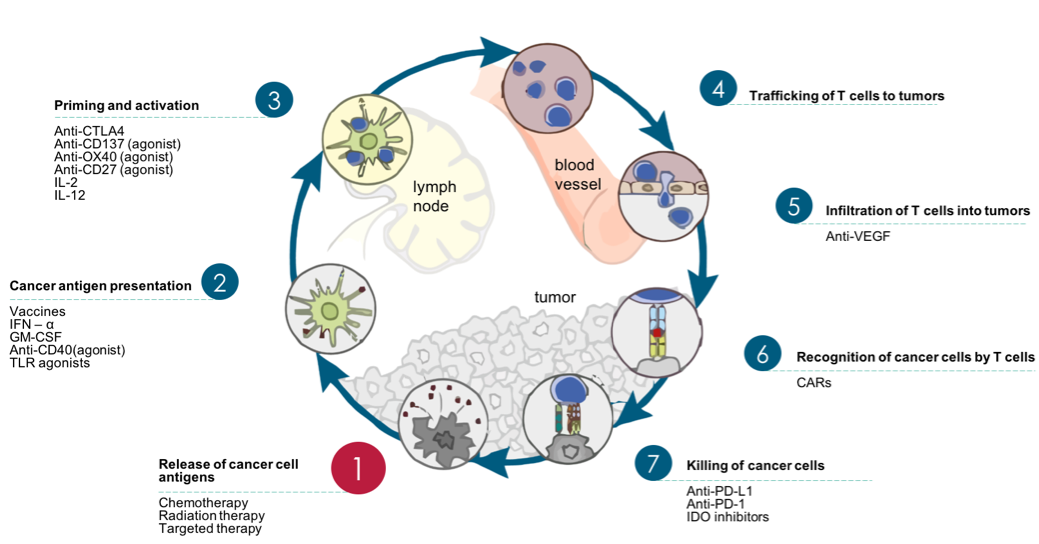
Key highlights are that vaccines can primarily promote cycle step 2, anti-CTLA4 can primarily promote cycle step 3, anti-PD-L1 or anti-PD-1 antibodies can primarily promote cycle step 1, and inhibitors of VEGF can potentially promote T cell infiltration into tumor-cycle step 5.
In our next article, we’ll talk about the immune-related response criteria and the guidelines for the evaluation of immune therapy activity in solid tumors by Dr. Jedd Wolchok.